




Expert Perspectives on Shoulder Instability

Dr. William N. Levine
One of the most common conditions of the upper extremity, glenohumeral instability has been a major focus of the orthopedic surgeons at NewYork-Presbyterian/Columbia University Irving Medical Center. Under the direction of William N. Levine, MD, Orthopedic Surgeon-in-Chief, Columbia Orthopedics has garnered a global reputation for clinical and research expertise in shoulder instability, helping to shape the transformation in surgical treatment from open repair and reconstruction to arthroscopic management over the past two decades.
The following article presents recent research by Columbia faculty that continues to innovate approaches to care for patients presenting with acute or chronic instability.
Epidemiology of Shoulder Instability in the National Football League
Shoulder instability is a common and potentially debilitating injury among collision-sport athletes that can lead to long-term damage of the glenohumeral joint. However, few studies have investigated the occurrence of shoulder instability among elite athletes in the National Football League (NFL). Columbia orthopedic surgeons retrospectively reviewed the NFL’s injury database for shoulder instability injuries resulting in missed time, classifying injuries by type (subluxation vs. dislocation), direction, timing (pre-season vs. regular season vs. post-season), setting (practice vs. game vs. conditioning), and injury mechanism. Median missed time was determined for the different types and directions of instability, and incidence rates were calculated based on timing and player position. Finally, the relationship between player position and instability direction was assessed.
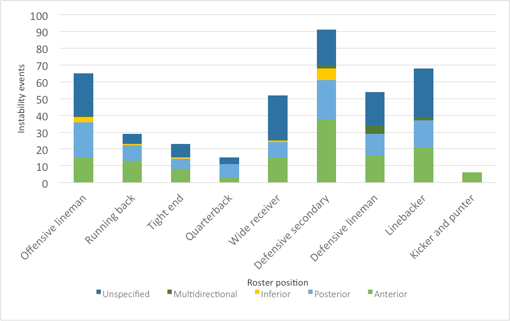
From 2012-2017, 355 players sustained 403 missed-time shoulder instability injuries. Most injuries occurred during games (65 percent) via a contact mechanism (85 percent). The overall incidence rate of game-related instability was 3.6 injuries per 100,000 player-plays and was highest during the pre-season. Defensive secondary accounted for the most injuries overall, but quarterbacks had the highest incidence rate in games (5.5 injuries per 100,000 player-plays). Approximately 70 percent of injuries were subluxations (n=192) while 30 percent were dislocations (n=83); 75 percent of dislocations were anterior while subluxations were more evenly distributed between anterior and posterior (45 percent vs. 52 percent, respectively). The majority of instability events among quarterbacks and offensive linemen were posterior (73 percent and 53 percent, respectively) while anterior instability was most common for all other positions. Players missed substantially more time following dislocation compared to subluxation (median of 47 days vs. 13 days, respectively).
The researchers concluded that shoulder instability is a common injury in the NFL, which can result in considerable missed time. Dislocations were noted to occur less frequently than subluxations but resulted in greater missed time. Certain player positions were associated with increased risk for shoulder instability, and player position also influenced instability direction.
The high incidence of posterior instability among offensive linemen and quarterbacks was attributed to repetitive microtrauma to the posterior capsulolabral complex sustained during position-specific motions such as blocking and throwing. Overall, this study highlights the diverse nature of shoulder instability injuries and the need for heightened awareness among medical personnel treating collision-sport athletes.
Shoulder Instability Direction by Roster Position
Read more:
Anderson M, Mack CD, Herzog MM, Levine WN. The epidemiology of shoulder instability in the National Football League. Orthopedic Journal of Sports Medicine. [In press 6/26/20]
To request the full text, please email: [email protected]
Shoulder Instability in the Professional Ice Hockey Player
The shoulder is a commonly injured area in hockey due to direct or indirect high-speed collisions with other players, collisions with the surrounding boards or equipment, and the aggressive nature of the game. Shoulder dislocations present a unique challenge to the competitive athlete as prompt management and treatment can be critical to career longevity and athletic performance. With a paucity of data examining its impact on hockey players and even less data available on outcomes in professional hockey players, Columbia orthopedic surgeons examined the incidence of shoulder dislocation events in the National Hockey League (NHL) and the effects on return-to-play and player performance. Their study is one of the first investigations on post-injury performance in professional hockey.
The retrospective cohort study evaluated NHL players who suffered at least one in-season shoulder instability event – defined as a dislocation of the glenohumeral joint requiring reduction – between the 2003-2004 and 2017-2018 seasons. The researchers collected demographic characteristics, incidence of injury, recurrences, return-to-play, and statistical performance data and compared post-injury performance with experience-matched, era-matched, position-matched, and age-matched controls. They used a mixed generalized linear regression model to compare post-injury performance as a function of operative and nonoperative treatment.
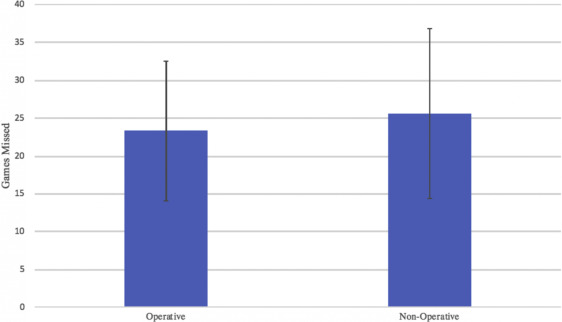
In the study, 57 players experienced 67 shoulder instability events with 98.5 percent of players returning to play after an average of 26.3 ± 20.8 regular season games missed. Surgery was performed in 47.8 percent of players with no recurrent injuries postoperatively. Nonoperatively managed players experienced a decrease in points per game compared with surgically treated patients. Recurrence occurred in 14.3 percent of conservatively managed players, with 33.3 percent experiencing a season-ending injury. The researchers also found that players with recurrent injuries missed significantly more career games compared with those treated initially with surgery.
The Columbia investigators concluded that professional hockey players experience high rates of return to play with acceptable performance outcomes after shoulder instability events. However, recurrent injuries led to significantly more career games missed when players were treated nonoperatively at the time of injury. Given the physical and financial impact of this type of injury on professional players, the authors believe there is a need to develop a treatment protocol for shoulder instability in hockey.
Average Number of Games Missed Based on Treatment Type
Read more:
Swindell HW, McCormick KL, Tedesco LJ, Herndon CL, Ahmad CS, Levine WN, Popkin CA. Shoulder instability, performance, and return to play in National Hockey League players. JSES International. 2020 Sep 22;4(4):786-791.
Coracoacromial Arch Anatomy and Anterior Shoulder Instability: Is There a Connection?
While glenoid bone loss and humeral head bone loss are well recognized as risk factors for recurrent instability, few studies looked at coracoacromial arch anatomy in the pathogenesis of glenohumeral instability.
With their hypothesis that coracoacromial arch anatomy is related to anterior shoulder instability, Columbia orthopedic surgeons undertook a retrospective cohort study of 50 patients with unidirectional anterior shoulder instability matched to a control group of 50 glenohumeral arthritis patients without any history of shoulder instability. They note that shoulders with a flatter roof of the coracoacromial arch likely have less overall containment of the humeral head in the sagittal plane. To their knowledge, this is the first study to measure the coracoacromial arch anatomy of patients with anterior shoulder instability and evaluate the relationship between shoulder arch morphology and the presence and severity of recurrent anterior instability.
To quantitatively measure and analyze the anatomy of the shoulder coracoacromial arch, nine radiographic measurements of the coracoacromial arch anatomy were taken in patients with unidirectional anterior shoulder instability or glenohumeral osteoarthritis:
- shoulder arch angle
- scapular Y angle
- anterior coracoid tilt
- posterior acromial tilt
- anterior acromial coverage angle
- posterior acromial angle
- coracoid height
- posterior acromial height
- critical shoulder angle
These measurements were determined using standard lateral scapular and anteroposterior radiographs.
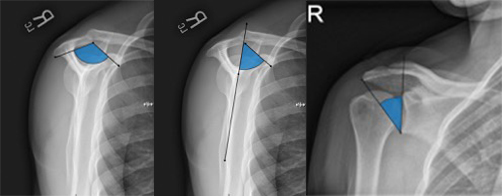
(Left) Measurement of the shoulder arch angle involves the angle formed by connecting 3 points: the posterior-inferior corner of the acromion, the most anterior-inferior corner of the acromion, and the most inferior edge of the coracoid. (Center) Measurement of the anterior coracoid tilt angle is formed by a vertical line through the center of the glenoid and scapular body and the anterior undersurface of the coracoid. (Right) Measurement of the critical shoulder angle involves the angle between the line parallel to the glenoid and the line from the inferior most aspect of the glenoid to the lateral most edge of the acromion.
The researchers found a significant association between the presence of instability and two of the measured anatomic factors: shoulder arch angle and critical shoulder angle. They also found a significant association between a larger anterior coracoid tilt and the presence of instability. However, a significant negative association was identified between instability and the posterior acromial coverage angle and the posterior acromial tilt.
This study identifies the shoulder arch angle and the anterior coracoid tilt as risk factors for anterior instability, as patients with a less contained coracoacromial arch were associated with anterior instability requiring arthroscopic stabilization. Greater posterior acromial coverage and posterior acromial tilt were also associated with reduced anterior shoulder instability contributing to the concept that the entire arch, both anteriorly and posteriorly, is important for stability. The findings suggest that this simple radiographic measurement method can be employed in routine orthopedic care to analyze risk and improve clinical decision making for shoulder instability.
Read more:
Lopez CD, Ding J, Bixby EC, Lobao MH, Heffernan JT, Levine WN, Jobin CM. Association between shoulder coracoacromial arch morphology and anterior instability of the shoulder. JSES International. 2020 Aug 21;4(4):772-779.
A Review Course on Shoulder Instability
Levine WN, Makhni EC, Athwal GS, Tokish JM. Technical pearls for shoulder instability. Instructional Course Lectures. 2021;70:23-36.
The goal of this review is to provide technical “pearls” in management of glenohumeral instability, including treatments such as arthroscopic anterior and posterior instability repair, posterior glenoid bone augmentation, open coracoid transfer (Latarjet) for anterior instability with bone loss, and complications related to coracoid transfer.
To request the full text, please email: [email protected].