




Minimally Invasive Surgery Offers More with Less

Dr. Eric H. Elowitz

Dr. Michael S. Virk
At the Center for Comprehensive Spine Care at NewYork-Presbyterian/Weill Cornell Medical Center, neurosurgeons Eric H. Elowitz, MD, and Michael S. Virk, MD, PhD, are taking advantage of the many techniques and technologies now available in minimally invasive spine surgery. “I have been performing minimally invasive spine surgery for the last 15 years and achieving the same goals or even better than with conventional open surgeries,” says Dr. Elowitz. “The area in which we’re seeing explosive growth is endoscopic surgery. This approach allows us to do spinal decompressions, as well as discectomies, with 7mm incisions via tissue and muscle-sparing corridors through natural openings into the spinal canal. The endoscope is not much bigger than a No. 2 pencil and offers excellent visualization. Micro instruments enable us to remove herniated disks and bone spurs in an extremely minimally invasive way.”
As Dr. Elowitz notes, indications for endoscopic spinal surgery are expanding, primarily in the lumbar region. “There are some instances where I can perform an endoscopic procedure as opposed to doing a fusion, which is a much bigger operation,” he says. “There is a select group of patients with a particular type of nerve pain that can be relieved with endoscopic surgery, thereby avoiding or delaying fusion surgery. I can also foresee in the not too distant future performing endoscopic spinal fusions with patients being able to go home the same day.”
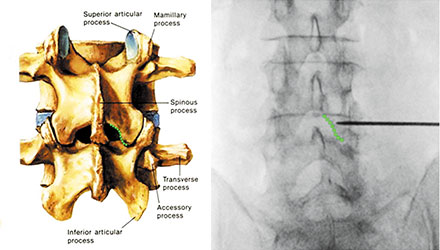
Target site – inferomedial edge of the lamina – is identified with fluoroscopy imaging.
“Certain revision cases or cases that are technically complex may require an open procedure, but my first approach is to accomplish our goals in a minimally invasive fashion,” says Dr. Virk.
Weill Cornell spine surgeons often take a circumferential approach to the spine. “We are pushing the envelope of performing extended applications for complex pathologies through smaller corridors,” he says. “Using an anterior approach, we can access the retroperitoneal space through an abdominal incision, or use a thoracic approach into the lateral corridor, going through the flank or between the ribs, and then performing percutaneous posterior instrumentation. Circumferential approaches generally involve multiple small incisions versus one extended incision in the back and this often translates into less global tissue disruption.”
Some of the approaches call on established collaborations with other surgical specialists. “For extended anterior approaches to the cervical spine, I have an ENT partner, Dr. Babak Sadoughi,” says Dr. Virk. “These cases may address complex deformity, tumors, or revisions and may require larger openings with more tissue mobilization, and his skills in this region help facilitate these cases.”
For anterior retroperitoneal lumbar approaches, Dr. Virk enlists the expertise of a Weill Cornell vascular surgeon, Dr. Sharif Ellozy. “He can mobilize the aorta or vena cava to provide access to the front of the spine,” he says. “Once a narrow corridor is established, we come in and do what we have to do.”