




Coronary Artery Disease
The interventional cardiologists and cardiac surgeons at NewYork-Presbyterian offer the most advanced percutaneous coronary interventions and coronary bypass programs in the world. Utilizing a range of approaches, from minimally invasive catheter-based treatments to off-pump coronary artery bypass to multiple arterial revascularization, they continually expand the boundaries of care for patients with coronary artery disease.
Lowering Bleeding Risk for Patients Undergoing Coronary Stent Procedures
While drug-eluting stents are the current standard for percutaneous coronary intervention, these stents necessitate longer durations of dual antiplatelet therapy (DAPT), potentially increasing bleeding in patients predisposed to these complications. Our physicians participated in the LEADERS FREE study to evaluate a polymer-free and carrier-free drug-coated stent that transfers umirolimus into the vessel wall over a period of one month. In a randomized, double-blind trial, they compared the drugcoated stent with a very similar bare-metal stent in patients with a high risk of bleeding. The results, published in The New England Journal of Medicine, demonstrated that the coated stent was superior to the bare-metal stent when used with a one-month course of DAPT.
NewYork-Presbyterian physicians are also leading the international ONYX ONE randomized controlled trial and the EVOLVE Short DAPT study, examining shorter durations of DAPT in conjunction with the use of the Onyx and Synergy drug-eluting stents. They are also about to begin enrollment in the XIENCE Short DAPT study, another trial examining a shorter duration of DAPT in patients at higher risk of bleeding.
Acute Myocardial Infarction
STEMI Performance Measures

Source: American College of Cardiology National Cardiovascular Data Registry
(ACTION Registry®-GWTG™) / Institutional Outcomes Report 2016
Publish Date: April 12, 2016
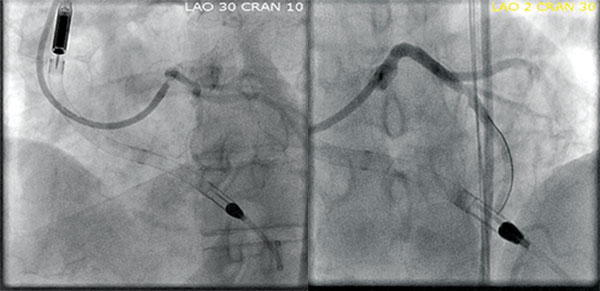
Case Study
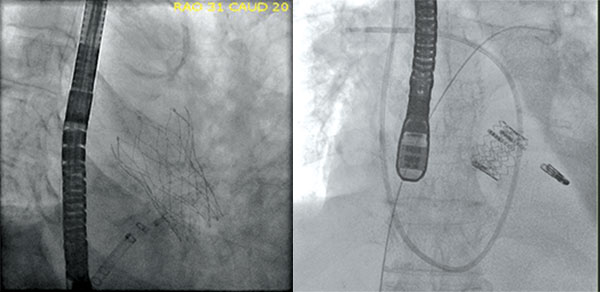
A female patient in her 50s underwent mantle field radiation for lymphoma as a child. She subsequently developed aortic stenosis and left main coronary artery stenosis. The patient’s left main lesion was addressed with a stent and an LVAD in the event she became hypotensive during the procedure, which could be fatal. Following recovery from this procedure, she then underwent TAVR with excellent results.
Stent and LVAD Placement
TAVR
Hybrid Coronary Revascularization
NewYork-Presbyterian has one of the finest programs in the nation for hybrid coronary revascularization that enables our surgeons to provide a combination of therapies for patients with extensive, multi-vessel disease. This approach combines minimally invasive robotic bypass off-pump, with the remaining arteries managed with stent placement. This technique brings the mammary artery to the left anterior descending artery without the need for cardiopulmonary bypass or sternotomy. NewYork-Presbyterian is a coordinating center for an actively enrolling NIH-sponsored, multicenter trial comparing hybrid coronary revascularization to conventional PCI.
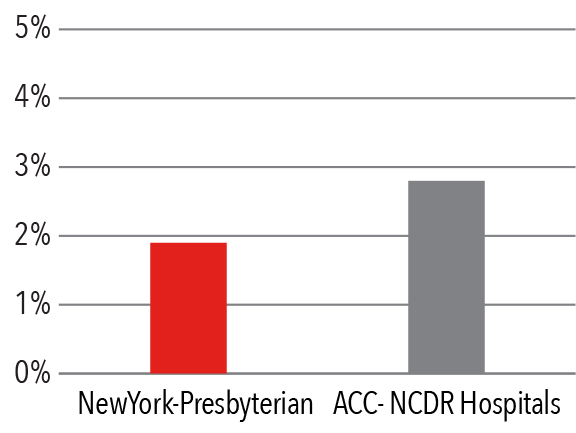
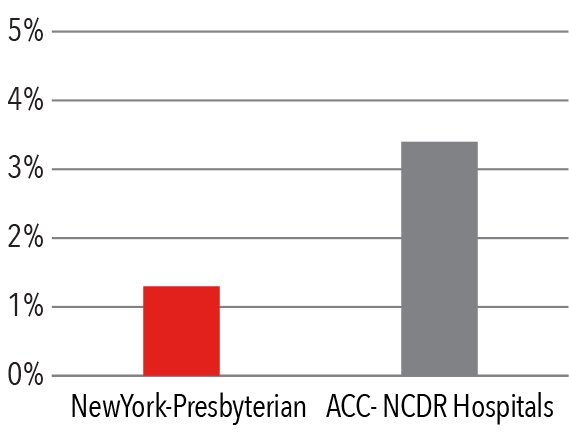
Percutaneous Coronary Intervention
Mortality Rate
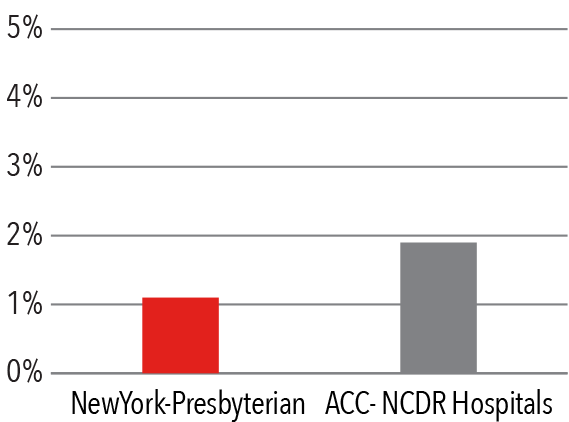
Source: American College of Cardiology
National Cardiovascular Data Registry (ACC-NCDR)
CathPCI Registry Institutional Outcomes Report 2016
Publish Date: April 12, 2016
Risk Factors of Patients Undergoing PCI
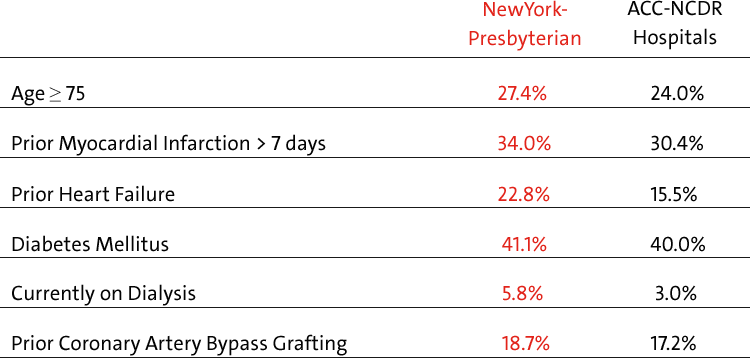
Source: American College of Cardiology National Cardiovascular Data Registry (ACC-NCDR)
CathPCI Registry Institutional Outcomes Report 2016
Publish Date: April 12, 2016
All Adverse Events*
Composite of adverse events – death, emergency
CABG, stroke, repeat target vessel revascularization Source: American College of Cardiology
National Cardiovascular Data Registry (ACC-NCDR) CathPCI Registry Institutional Outcomes Report 2016
Publish Date: April 12, 2016
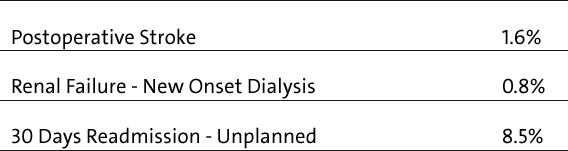
PCI Complications — Incidents per Total Volume
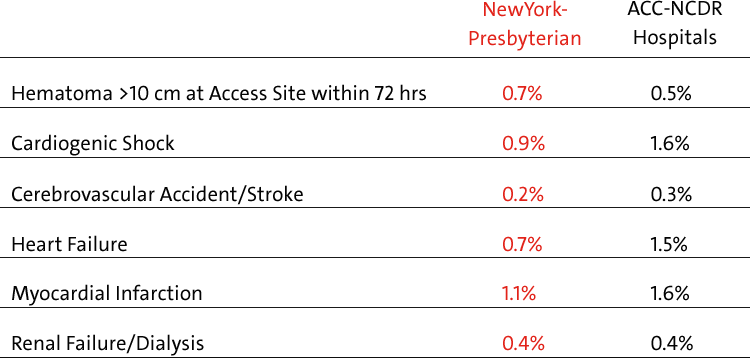
Source: American College of Cardiology National Cardiovascular Data Registry (ACC-NCDR)
CathPCI Registry nstitutional Outcomes Report 2016
Publish Date: April 12, 2016
Current Perspectives on CABG
While the use of the left internal mammary artery is a standard expectation for coronary artery byass grafting, our cardiothoracic surgeons are using multiple arterial grafts, as opposed to vein grafts, for their durability and the expectation of greater longevity, especially beneficial for younger patients. The graft conduits include the bilateral mammary artery, the radial artery, and the gastroepiploic artery.
With our experience and expertise caring for high-risk patients, we are able to perform bypass surgery on patients with the most complex and challenging cardiac disease using ventricular assist devices, ECMO, and advanced pharmacology.
-
In January 2018, Weill Cornell will serve as the principal investigating institution for the multicenter ROMA (Randomization of Single Multiple Arterial Grafts) trial that will compare the clinical outcome of single versus multiple arterial grafts in patients undergoing primary isolated non-emergent coronary artery bypass grafting. The ROMA trial – expected to be the second largest clinical trial conducted for coronary bypass – aims to enroll nearly 4,500 patients in six continents over the next three years.
-
NewYork-Presbyterian uses bilateral internal mammary arteries for a much higher proportion of patients than almost any other institution in the country. In the most recent national surveys, only 5 to 10 percent of patients receive bilateral mammary grafts for coronary bypass in the United States; at NewYork-Presbyterian, more than 60 percent of our patients benefit from this approach.
-
Our surgeons use other methods for multiple arterial grafting, such as sequential grafting that involves one arterial conduit to bypass multiple targets; less commonly, they employ branch grafting with the Y-graft or T-graft.
-
When performing complex radial grafts, collateral blood flow to the hands and fingers following revascularization is carefully evaluated to minimize ischemia to the hand. Rigorous diagnostic assessment in the operating room includes the use of ultrasound and transit time flowmeters to confirm good flow and graft patency.
-
To preserve sternal blood flow and minimize the risk of sternal infection, our surgeons skeletonize the mammary arteries. Instead of taking all of the tissues and veins around the artery, they take only the artery, preserving blood flow to the sternum as much as possible.
Coronary Artery Bypass Grafting
2016 Volume
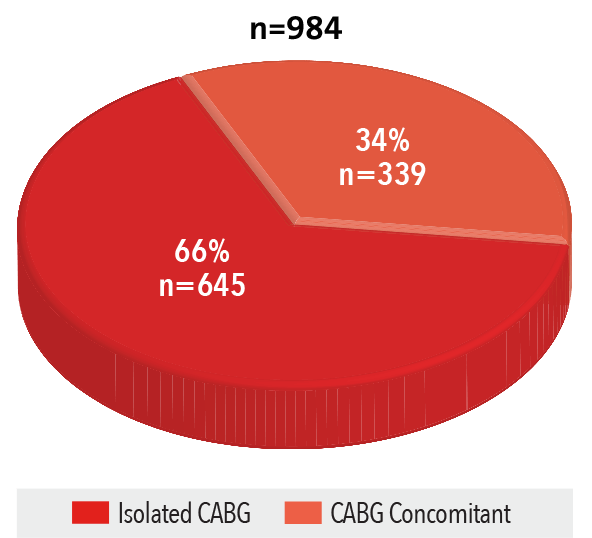
Source: NewYork-Presbyterian
30-Day Mortality Rate
July 1, 2013 - June 30, 2016
Source: Hospital Compare (of 1,194 hospitals in the U.S.)
Isolated CABG Complications Rate
2014 - 2016
Source: Vizient Clinical Data Base/Resource Manager™ used by permission of Vizient. All rights reserved.