




With campuses located throughout New York City, pulmonologists and critical care specialists at NewYork-Presbyterian managed an extraordinary number of cases and range of disease severity in patients with COVID-19. In the year since the pandemic began to unfold, clinicians and scientists worldwide have produced research on all aspects of the virus at a record pace hoping to stem its appalling rates of mortality and associated morbidities.
The pulmonology faculty at NewYork-Presbyterian’s affiliated medical schools – Columbia University Vagelos College of Physicians and Surgeons and Weill Cornell Medicine – then and now – are among the many specialists applying their clinical and investigational skills to understand the virus and its repercussions in patients and identify therapies that are appropriate and successful in patients along the virus’s spectrum of severity.
Evaluation and Management of Patients with Severe COVID-19
In the December 17, 2020 issue of The New England Journal of Medicine, Weill Cornell pulmonary and critical care specialists provide a detailed analysis of caring for a patient with severe COVID-19 who became critically ill with acute respiratory distress syndrome. The various strategies they present include the basics of respiratory care, endotracheal intubation; ventilator management; caring for patients with refractory hypoxemia; therapies, including dexamethasone and remdesivir; and supportive care. The authors conclude with their recommendations for care. Given the high risk of complications from severe COVID-19, the clinicians also advise physicians to work with patients and families to establish appropriate goals of care at the earliest possible time.
Read more:
Berlin DA, Gulick RM, Martinez FJ. Severe COVID-19. The New England Journal of Medicine. 2020 Dec 17;383(25):2451-2460.
Emerging Data on the Role of ECMO for COVID-19
Daniel Brodie, MD, Director, Adult ECMO Program, and Director, Center for Acute Respiratory Failure, at NewYork-Presbyterian/Columbia, and colleagues from health systems in Singapore and Paris, report on the current status of extracorporeal membrane oxygenation (ECMO) in the treatment of patients critically ill with COVID-19. Studies from China in the early days of the pandemic reported high mortality rates in patients supported with ECMO. With little known about the virus at the time, the value of using ECMO was uncertain. Now, nearly one year out from the earliest reported cases, studies out of the U.S. and France have demonstrated that ECMO appears to have a role in the management of adult patients with COVID-19 who suffer from ARDS refractory to other management strategies.
The new data tempers the initial concerns that ECMO for COVID-19 was associated with unacceptable short-term outcomes particularly when used in experienced centers. Longer term data is now needed to answer questions such as:
- Are the longer ECMO runs seen in COVID-19 associated with an increase in the risk of ECMO-related complications and morbidity, e.g. nosocomial infection?
- Is there an increase in bleeding or thrombotic complications despite optimal anticoagulation and is this associated with an increase in the risk of mechanical circuit problems or failure?
- What are the long-term outcomes of patients with COVID-19 supported with ECMO?
- What is the maximum duration of ECMO where recovery is still possible and is lung transplantation an option beyond that?
Read more:
MacLaren G, Combes A, Brodie D. What's new in ECMO for COVID-19? Intensive Care Medicine. 2021 Jan;47(1):107-109.
A Global and In-Depth Report on COVID-19 and COPD
As a member of the Global Initiative for Chronic Obstructive Lung Disease (GOLD) Science Committee, Fernando J. Martinez, MD, Chief of the Pulmonary and Critical Care Medicine Division, NewYork-Presbyterian/Weill Cornell, contributed to a report on caring for patients with COPD during the COVID-19 pandemic. The SARS-CoV-2 pandemic has raised a number of questions about the management of these patients and whether patients with COPD are at increased risk of becoming infected with SARS-CoV-2. Using established methods for literature review, the researchers present guidelines that include:
- Risk of infection for patients with COPD
- Testing recommendations, including spirometry and bronchoscopy
- Protective strategies for patients with COPD
- Differentiating COVID-19 infection from daily symptoms of COPD
The committee also discusses pharmacological and nonpharmacological treatment for COPD during the pandemic; pulmonary and extrapulmonary complications; ventilatory support for patients with COPD and COVID-19 pneumonia; and rehabilitation and follow-up of patients with COPD who developed COVID-19.
Read more:
Halpin DMG, Criner GJ, Papi A, Singh D, Anzueto A, Martinez FJ, Agusti AA, Vogelmeier CF. Global Initiative for the Diagnosis, Management, and Prevention of Chronic Obstructive Lung Disease. The 2020 GOLD Science Committee Report on COVID-19 and Chronic Obstructive Pulmonary Disease. American Journal of Respiratory and Critical Care Medicine. 2021 Jan 1;203(1):24-36.
Autopsies Reveal the Spectrum of Pathology in COVID-19 Patients
Columbia researchers in the Departments of Pulmonary, Allergy and Critical Care Medicine, Pathology and Cell Biology, Radiology, and Pharmacy collaborated on a review of 40 postmortem examinations from COVID-19 decedents to evaluate the spectrum of pathology and correlate the results with clinical, laboratory, and radiologic findings. Although diffuse alveolar damage, a subtype of acute lung injury (ALI), is the most common microscopic pattern in COVID-19, other pathologic patterns have been described. The researchers noted two distinct pulmonary phenotypic patterns – ALI and non-ALI. Non-ALI represents a rarely described phenotype, and they note that cause of death in non-ALI is most likely COVID-19 related but will require additional corroboration.
Read more:
De Michele S, Sun Y, Yilmaz MM, Katsyv I, Salvatore M, Dzierba AL, Marboe CC, Brodie D, Patel NM, Garcia CK, Saqi A. Forty postmortem examinations in COVID-19 Patients. American Journal of Clinical Pathology. 2020 Nov 4;154(6):748-760.
COVID-19: A Roadmap for Hospital Preparedness
Collaboration among pulmonary and critical care medicine specialists at NewYork-Presbyterian/Weill Cornell Medical Center and their colleagues in the departments and divisions of anesthesiology, cardiology, neurocritical care, surgical critical care, hospital medicine, infectious diseases, palliative care, ethics, nursing, physical therapy, and respiratory therapy formed the foundation for expanding caregiving capabilities and meeting the challenges of the COVID-19 pandemic. In their comprehensive article, the authors present a critical care perspective on preparing for the first wave of the pandemic with potential guidelines for other centers to adapt as needed going forward to meet the ongoing inpatient challenges related to patients with COVID-19. Topics covered include surge planning and clinical operational challenges, as well as protocols for clinical decision-making on areas such as intubation, use of high-flow oxygen, and cardiac arrest.
Read more:
Griffin KM, Karas MG, Ivascu NS, Lief L. Hospital preparedness for COVID-19: A practical guide from a critical care perspective. American Journal of Respiratory and Critical Care Medicine. 2020 Jun 1;201(11):1337-1344..
Research from the Early Days of the Pandemic
Getting a Handle on Clinical Course
During March 2 and April 1, 2020, as patients presenting to hospitals with COVID-19 began to quickly escalate, Columbia faculty undertook a prospective observational cohort study at two affiliated NewYork-Presbyterian hospitals in northern Manhattan.
The researchers identified 1,150 adults admitted with laboratory-confirmed COVID-19, of which 257 (22 percent) were critically ill with acute hypoxemic respiratory failure. Their evaluation of clinical, biomarker, and treatment data focused primarily on rate of in-hospital death, followed by frequency and duration of invasive mechanical ventilation, frequency of vasopressor use and renal replacement therapy, and time to in-hospital clinical deterioration following admission.
Follow-up continued to April 28, 2020, so that each patient had at least 28 days of observation. As of that date, 101 (39 percent) patients had died and 94 (37 percent) remained hospitalized. Older age, chronic cardiac disease, chronic pulmonary disease, higher concentrations of interleukin-6, and higher concentrations of D-dimer were independently associated with in-hospital mortality.
Of the 1,150-patient cohort, the researchers noted the following:
- 212 (82 percent) had at least one chronic illness, most commonly hypertension, diabetes, and obesity
- Median time to in-hospital deterioration was 3 days
- 203 (79 percent) patients received invasive mechanical ventilation for a median of 18 days
- 170 (66 percent) of 257 patients critically ill at admission received vasopressors and 79 (31 percent) received renal replacement therapy
The Columbia study confirmed that critical illness among patients hospitalized with COVID-19 in New York City was common and associated with a high frequency of invasive mechanical ventilation, extrapulmonary organ dysfunction, and substantial in-hospital mortality.
Weill Cornell Medicine faculty had similar findings in their review of the first 393 consecutive patients admitted to two affiliated NewYork-Presbyterian hospitals in midtown and lower Manhattan between March 3 and March 27, 2020. Ninety percent of the patients had lymphopenia, 27 percent had thrombocytopenia, and many had elevated liver-function values and inflammatory markers. Between March 3 and April 10, respiratory failure leading to invasive mechanical ventilation developed in 130 patients (33.1 percent); as of the writing of the paper, only 43 of these patients (33.1 percent) had been extubated. In total, 40 of the patients (10.2 percent) have died, and 260 (66.2 percent) have been discharged from the hospital; outcome data are incomplete for the remaining 93 patients (23.7 percent).
The researchers observed that obesity was a common characteristic and may be a risk factor for respiratory failure leading to invasive mechanical ventilation. In addition, they note that the patients who received invasive mechanical ventilation almost universally received vasopressor support and that many also received renal replacement therapy.
Read more:
Cummings MJ, Baldwin MR, Abrams D, Jacobson SD, Meyer BJ, Balaough EM, Aaron JG, Classen J, Rabbani LE, Hastie J, Hochman BR, Salazar-Schicchi J, Yip NH, Brodie D, O’Donnell MR. Epidemiology, clinical course, and outcomes of critically ill adults with COVID-19 in New York City: a prospective cohort study. The Lancet. 2020 Jun 6; 395(10239): 1762-70.
Goyal P, Choi JJ, Pinheiro LC, Schenck EJ, Chen R, Jabri A, Satlin MJ, Campion TR Jr, Nahid M, Ringel JB, Hoffman KL, Alshak MN, Li HA, Wehmeyer GT, Rajan M, Reshetnyak E, Hupert N, Horn EM, Martinez FJ, Gulick RM, Safford MM. Clinical characteristics of COVID-19 in New York City. The New England Journal of Medicine. 2020 Jun 11;382(24):2372-74.
Atypical Respiratory Distress
Is the respiratory distress syndrome accompanying a subset of severe COVID-19 distinct from classic acute respiratory distress syndrome? Weill Cornell and Columbia pulmonologists in collaboration with pathologists examined this question in studies at their respective campuses.
At Weill Cornell, the physicians noted that in patients with COVID-19, there is relatively well-preserved lung mechanics despite the severity of hypoxemia and increasing recognition of systemic features of a hypercoaguable state suggesting the pathology and pathophysiology of COVID-19 might differ from that of typical acute respiratory distress syndrome. They examined five cases of persistent, severe COVID-19 in seeking to define the role of complement activation and microvascular thrombosis.
All 5 patients were selected for pathologic studies based on a respiratory tract sample positive for SARS-CoV-2 in a reverse transcriptase-polymerase chain reaction assay. They represent the first two patients succumbing to COVID-19 and undergoing autopsy that were available to the physicians, and the first three infected individuals for whom a dermatologic consult had been requested to evaluate an extensive skin rash.
From the examination of pulmonary and cutaneous biopsy and autopsy samples, the physicians documented that at least some SARS-CoV-2-infected patients who become critically ill suffer a generalized thrombotic microvascular injury. Such pathology involves at least the lung and skin, and appears mediated by intense complement activation. Their histologic findings were consistent with emerging observations suggesting that COVID-19 has clinical features distinct from typical ARDS.
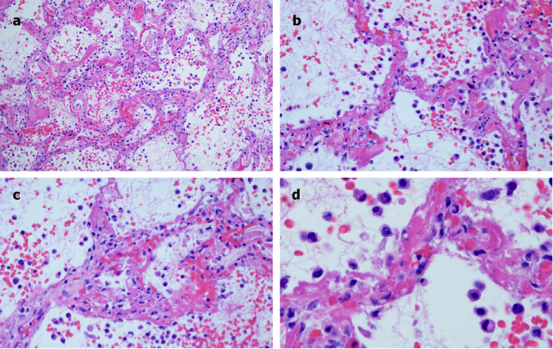
Microscopic features of pulmonary autopsy samples from Case 2 show (A) Extensive hemorrhagic pneumonitis with red cell extravasation and fibrin in alveolar spaces and luminal and mural fibrin deposition within septal capillaries (B) The septa exhibiting a pauci-cellular pattern of capillary injury as evidenced by significant fibrin deposition, with thrombi seen in capillaries; there is red cell extravasation in the alveolar spaces along with collections of neutrophils and monocytes (C) A slight widening of the septa by a few inflammatory cells, predominantly neutrophils and evidence of capillary injury characterized by fibrin deposition in the lumens and walls with red cell extravasation within the septa and adjacent alveolar space (D) With higher power examination, capillary wall disruption accompanied by fibrin deposition and red cell extravasation, with neutrophils in the septa and within the alveolar spaces is further illuminated.
In addition, Weill Cornell pathologists collaborated with colleagues in two other institutions significantly affected by the pandemic – another in New York City and one in Italy – to determine the range of pulmonary pathology involved in SARS-CoV-2. Their detailed examination of 68 consecutive COVID-19 autopsies showed a consistent pattern of tracheobronchitis, alveolar injury, and vascular/thrombotic disease in patients with frequent co-morbidities such as hypertension and diabetes, as well as a high frequency of thrombi, especially platelet thrombi. Several compartments were involved, from upper airways (trachea, bronchi) to lung parenchyma, and the vascular bed. The study’s authors note that clinical and histologic findings were similar among the three institutions despite differing patient populations between the Italian and US cohorts.
At Columbia, researchers pursued a study on respiratory pathology beyond diffuse alveolar damage, which has been the most common microscopic pattern in COVID-19. To characterize these outlier patterns, they undertook a comprehensive and quantitative review of 40 postmortem examinations to evaluate the spectrum of pathology and correlate the results with clinical, laboratory, and radiologic findings. All of the decedents had confirmed severe acute respiratory syndrome.
The research team’s review revealed three major pulmonary patterns: Acute lung injury (73 percent), intravascular fibrin or platelet-rich aggregates (90 percent), and vascular congestion (90 percent) and hemagiomatosis-like change (50 percent). There was also a cohort without acute lung injury, which suggested two main pulmonary pathologic phenotypes – ALI and non-ALI. The researchers further note that patients with a non-ALI phenotype represent a rarely described subgroup with a cause of death that may include cardiac and/or vascular pathways.
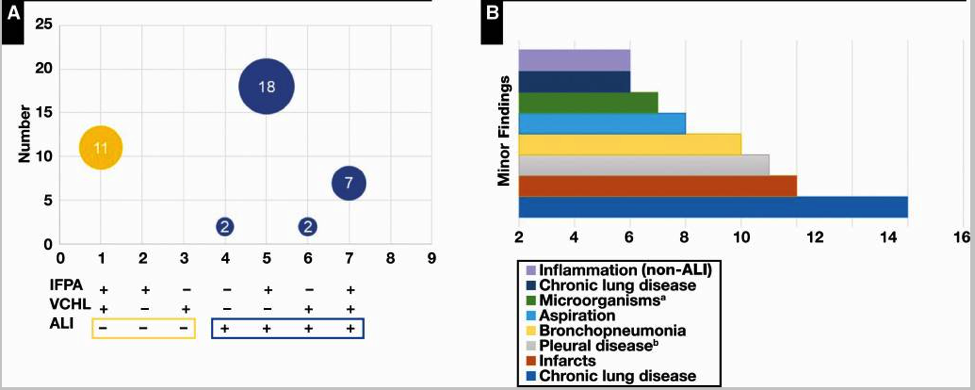
The spectrum of lung pathology in coronavirus disease 2019 was categorized as (A) major and (B) minor pathologic patterns. ALI, acute lung injury; IFPA, intravascular fibrin or platelet aggregate; VCHL, vascular congestion and hemangiomatosis-like change. a Candida species, herpes simplex virus, and Aspergillus species. b Congestion, fibrosis, or chronic inflammation.
Read more:
Magro C, Mulvey JJ, Berlin D, Nuovo G, Salvatore S, Harp J, Baxter-Stoltzfus A, Laurence J. Complement associated microvascular injury and thrombosis in the pathogenesis of severe COVID-19 infection: A report of five cases. Translational Research. 2020 Jun;220:1-13.
Borczuk AC, Salvatore SP, Seshan SV, Patel SS, Bussel JB, Mostyka M, Elsoukkary S, He B, Del Vecchio C, Fortarezza F, Pezzuto F, Navalesi P, Crisanti A, Fowkes ME, Bryce CH, Calabrese F, Beasley MB. COVID-19 pulmonary pathology: a multi-institutional autopsy cohort from Italy and New York City. Modern Pathology. 2020 Sep 2:1-13.
De Michele S, Sun Y, Yilmaz MM, Katsyv I, Salvatore M, Dzierba AL, Marboe CC, Brodie D, Patel NM, Garcia CK, and Saqi, A. Forty post-mortem examinations in Covid-19 patients: Two distinct pathologic phenotypes and correlation with clinical and radiographic findings. American Journal of Clinical Pathology. 2020 Sep 2:aqaa156.
Impact of Obesity on Respiratory Risk
Early on in the pandemic, obesity was revealed to be a risk factor for complications in COVID-19 for a number of reasons: adipocytes activate the inflammatory cascade, increasing risk for thromboembolism and susceptibility to the cytokine storm; negative affect on lung mechanics; and the potential to alter mitochondrial bioenergetics in lung epithelial cells and increase risk for acute lung injury.
Weill Cornell and Columbia faculty each conducted a retrospective review of patients to better understand the association between obesity, respiratory distress and failure, and in-hospital mortality. Both groups of researchers examined a diverse cohort of patients – more than 4,000 in total – hospitalized with confirmed COVID-19 at their respective quaternary academic medical center and community hospital campuses of NewYork-Presbyterian Hospital.
The retrospective observational cohort study at Weill Cornell included 1,687 adults with confirmed COVID-19 hospitalized between March 3 and May 15, 2020. The median BMI was 27 kg/m2; 31.1 percent were obese. The researchers found a J-shaped pattern for in-hospital mortality. The fully adjusted hazard of dying was highest for underweight persons, lowest for overweight persons, and progressively increased with higher degrees of obesity. For respiratory failure, the fully adjusted hazard ratio was lowest among persons with normal weight and progressively increased with higher BMI class. These findings indicated that obesity is an independent risk factor for respiratory failure but not for in-hospital mortality, and explain the extensive use of invasive mechanical ventilation reported in the United States, where the prevalence of obesity exceeds 40 percent.
At Columbia, researchers reviewed 2,466 adults hospitalized with laboratory-confirmed severe acute respiratory syndrome coronavirus 2 infection over a 45-day period with at least 47 days of in-hospital observation. Over a median hospital length of stay of 7 days, 533 patients (22 percent) were intubated, 627 (25 percent) died, and 59 (2 percent) remained hospitalized. Compared with overweight patients, patients with obesity had higher risk for intubation or death, with the highest risk among those with class 3 obesity. This association was primarily observed among patients younger than 65 years and not in older patients. Body mass index was not associated with admission levels of biomarkers of inflammation, cardiac injury, or fibrinolysis.
Read more:
Goyal P, Ringel JB, Rajan M, Choi JJ, Pinheiro LC, Li HA, Wehmeyer GT, Alshak MN, Jabri A, Schenck EJ, Chen R, Satlin MJ, Campion TR Jr, Nahid M, Plataki M, Hoffman KL, Reshetnyak E, Hupert N, Horn EM, Martinez FJ, Gulick RM, Safford MM. Obesity and COVID-19 in New York City: A retrospective cohort study. Annals of Internal Medicine. 2020 Jul 6:M20-2730.
Anderson MR, Geleris J, Anderson DR, Zucker J, Nobel YR, Freedberg D, Small-Sauders J, Rajagopalan KN, Greendyk R, Chae S, Natarajan K, Roh D, Edwin E, Gallagher D, Podolanczuk A, Barr RG, Ferrante AW, Baldwin MR. Body mass index and risk for intubation or death in SARS-CoV-2 infection: A retrospective cohort study. Annals of Internal Medicine. 2020 July 29:M20-3214.
Medication Management
Studying Hydroxychloroquine
Hydroxychloroquine has been widely administered to patients with COVID-19 without robust evidence supporting its use. Columbia physicians examined the association between hydroxychloroquine use and intubation or death from data obtained on 1,446 consecutive patients hospitalized with COVID-19, excluding those who were intubated, died, or discharged within 24 hours after presentation to the emergency department (study baseline). The primary end point was a composite of intubation or death in a time-to-event analysis. The physicians compared outcomes in patients who received hydroxychloroquine with those in patients who did not. They observed that hydroxychloroquine administration was not associated with either a greatly lowered or an increased risk.
Evaluating Convalescent Plasma
In a single center, phase 2, randomized, controlled trial, Columbia faculty are evaluating the efficacy and safety of human anti-SARS-CoV-2 convalescent plasma in hospitalized adults with severe SARS-CoV-2 infection. To procure the investigational treatment, volunteers who recovered from COVID-19 will undergo testing to confirm the presence of anti-SARS-CoV-2 antibody. The primary endpoint is time-to-clinical improvement and is defined as time from randomization to either discharge from the hospital or improvement by one point on a seven-point ordinal scale, whichever occurs first. The Columbia investigators plan to enroll 129 participants in the ongoing study, with 86 in the anti-SARS-CoV-2 arm, and 43 in the control arm.
Read more:
Geleris J, Sun Y, Platt J, Zucker J, Baldwin M, Hripcsak G, Labella A, Manson DK, Kubin C, Barr RG, Sobieszczyk ME, Schluger NW. Observational study of hydroxychloroquine in hospitalized patients with COVID-19. The New England Journal of Medicine. 2020 Jun 18;382(25):2411-2418.
Eckhardt CM, Cummings MJ, Rajagopalan KN, Borden S, Bitan ZC, Wolf A, Kantor A, Briese T, Meyer BJ, Jacobson SD, Scotto D, Mishra N, Philip NM, Stotler BA, Schwartz J, Shaz B, Spitalnik SL, Eisenberger A, Hod EA, Justman J, Cheung K, Lipkin WI, O’Donnell MR. Evaluating the efficacy and safety of human anti-SARS-CoV-2 convalescent plasma in severely ill adults with COVID-19: A structured summary of a study protocol for a randomized controlled trial. Trials. 2020 Jun 8:21(1):499.
Meeting Concerns of Respiratory Support
A Closer Look at Respiratory Mechanics
The COVID-19 pandemic has dramatically increased the number of patients requiring mechanical ventilation for respiratory failure. Several case series with data on ventilator variables from small cohorts had been reported, however, differences in respiratory mechanics between those with early mortality and successful extubation had not been explored. Weill Cornell Medicine physicians report on physiologic and clinical information from 267 patients with COVID-19 during the first week of mechanical ventilation. Their study summarizes the demographics, comorbidities, and intensive care unit treatments, as well as ventilator variables. The researchers concluded that patients in this cohort of COVID-19 respiratory failure met criteria for moderate-to-severe ARDS and had baseline respiratory mechanics that were comparable to those in patients enrolled in prior therapeutic trials and observational studies of ARDS.
Ventilator-Sharing Protocol
During the rapidly expanding pandemic, Columbia physicians joined with clinicians at other academic institutions in developing a novel ventilator sharing strategy to support two patients simultaneously with one ventilator. In an article in the August 15, 2020 issue of the American Journal of Respiratory and Critical Care, they reported on their initial ventilator sharing experience among patients with COVID-19-associated acute respiratory distress syndrome (ARDS). The authors detailed methods, patient selection, circuit configuration, safety features, patient management, and the statistical analysis of data recorded during and for 48 hours before and after ventilator sharing of three pairs of patients. Their report demonstrated the feasibility of ventilator sharing for COVID-19-associated ARDS. Following a rigorous clinical protocol, carefully selected patient pairs receiving continuous neuromuscular blockade tolerated ventilator sharing for two days without adverse events. The researchers concluded that in acute ventilator shortages, after exhausting alternatives, ventilator sharing is a reasonable stopgap to support potentially rescuable patients for at least two days in centers with appropriate expertise.
Implementing the Prone Position
Columbia faculty conducted a study to investigate whether the prone position is associated with improved oxygenation and decreased risk for intubation in spontaneously breathing patients with severe COVID-19 hypoxemic respiratory failure. The physicians screened 88 consecutive patients admitted to the step-down unit at NewYork-Presbyterian/Columbia between April 6 and April 14, 2020. They found that the use of the prone position for awake, spontaneously breathing patients with COVID-19 severe hypoxemic respiratory failure was associated with improved oxygenation. In addition, patients with an Spo2 of 95 percent or greater after one hour of the prone position was associated with a lower rate of intubation.
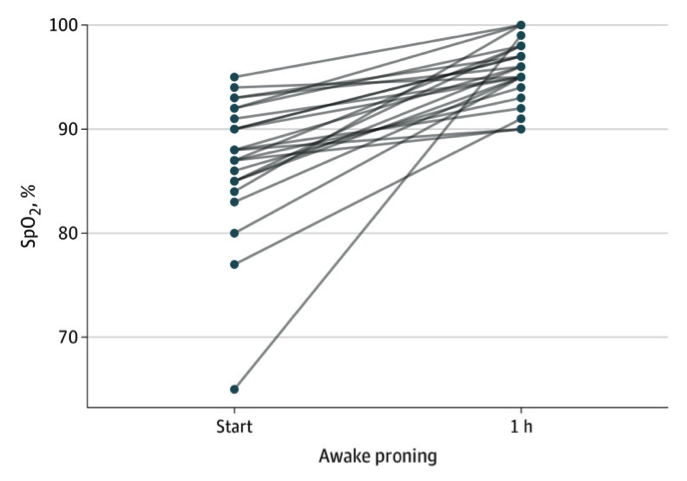
Oxyhemoglobin saturation (Spo2) one hour after initiation of the prone position in awake, nonintubated patients with COVID-19. One hour after initiation of the prone position, 19 patients had Spo2 of 95% or greater; subsequently, 7 (37%) required intubation.
Read more:
Thompson AE, Ranard BL, Wei Y, Jelic S. Prone positioning in awake, nonintubated patients with COVID-19 hypoxemic respiratory failure. JAMA Internal Medicine. 2020 Jun 17;e203030.
Beitler JR, Mittel AM, Kallet R, Kacmarek R, Hess D, Branson R, Olson M, Garcia I, Powell B, Wang DS, Hastie J, Panzer O, Brodie D, Hill LL, Thompson BT. Ventilator sharing during an acute shortage caused by the COVID-19 pandemic. American Journal of Respiratory and Critical Care. 2020 Aug o15;2020(4):600-04.
Schenck EJ, Hoffman K, Goyal P, Choi J, Torres L, Rajwani K, Tam CW, Ivascu N, Martinez FJ, Berlin DA. Respiratory mechanics and gas exchange in COVID-19-associated respiratory failure. Annals of the American Thoracic Society. 2020 Sep;17(9):1158-61.