




Colloid cysts of the third ventricle represent less than 1 to 2 percent of all intracranial tumors, occurring in only about one in three million people. While they have the potential for progressing, they typically grow at a very slow indolent rate. Sudden deterioration and death secondary to obstructive hydrocephalus are well-described presentations in patients with a colloid cyst. Although they can be found in children, they are typically diagnosed in adults in their thirties and forties.

Dr. Mark Souweidane
“Most neurosurgeons who do intracranial work probably see on the order of about two or three of these rare tumors in the course of their career,” says Mark M. Souweidane, MD, Vice Chairman of Neurological Surgery and a Professor of Neurological Surgery in Pediatrics at Weill Cornell Medicine and Director of Pediatric Neurological Surgery at NewYork-Presbyterian/
“Colloid cysts have challenged neurosurgeons for as long as neurosurgery has been a profession. While lesions in and around the third ventricle are certainly not off limits to neurosurgeons, the approach toward these cysts is extremely demanding and it takes an exceptional amount of technical prowess to even reach, let alone remove them,” says Dr. Souweidane.
Patients whose cysts were considered too dangerous to reach surgically were once advised to watch and wait, which increased the risk of sudden death. The newer endoscopic approach changes that equation and allows more patients to be treated, but few neurosurgeons are adept at this approach. Dr. Souweidane has performed more than 200 endoscopic surgeries to remove colloid cysts in children and adults, making him one of the world’s experts in this minimally invasive procedure.
Endoscopy images during colloid cyst surgery
Several factors determine the best treatment strategy for patients with a colloid cyst. Cyst size, the degree of cerebrospinal fluid blockage, and the age of the patient are all important features to consider in defining the best management plan. “I think most would agree that when a colloid cyst reaches a threshold of about 10 millimeters, that starts to raise a level of concern, given those patients who do deteriorate,” says Dr. Souweidane. “Young age is also a major consideration. If a patient is diagnosed early in life and has two, three, four, or five decades of life ahead of them, that's a long time to carry the risk of sudden death, so it makes sense to remove the cyst, especially if we can do it endoscopically."
“The endoscope has truly changed the playing field and the threshold in these patients and the colloid cyst lends itself very well to endoscopic removal owing to the cystic nature of it.” — Dr. Mark Souweidane
Dr. Souweidane’s plan of care for a 16-year-old versus an 86-year-old is very different based on the potential impact of the lesion. “My mindset is so different today than it was when I was in training some 20 years ago because the relative risk of our endoscopic surgical approach has plummeted,” he says. “The endoscope has truly changed the playing field and the threshold in these patients and the colloid cyst lends itself very well to endoscopic removal owing to the cystic nature of it. It is also very appropriate and safe to offer patients no surgery if they have absolutely no symptoms associated with their colloid cyst, if the ventricles are small and there is no relative blockage of fluid, and the cyst is below that threshold.”
Defining Differences in Children and Adults
The rarity of these benign tumors in children makes it difficult to differentiate and present meaningful information on treatment. To that end, Dr. Souweidane and Weill Cornell Medicine neurosurgical faculty led a multicenter study to define distinctive features of colloid cyst presentation, treatment, and outcome in children compared with adults. The results of their research were published in the April 23, 2021, issue of the Journal of Neurosurgery: Pediatrics.
Dr. Souweidane and Weill Cornell Medicine neurosurgical faculty led a multicenter study to define distinctive features of colloid cyst presentation, treatment, and outcome in children compared with adults.
In this study, the researchers conducted a retrospective review of patients with a colloid cyst of the third ventricle who underwent endoscopic surgery performed by Dr. Souweidane between 1999 and 2018. The reviewers analyzed patient demographic data, clinical presenting symptoms, radiological features, operative data, postoperative outcomes, and recurrence rates. Patients were grouped as pediatric (age ≤18 years) and adult (age >18 years).
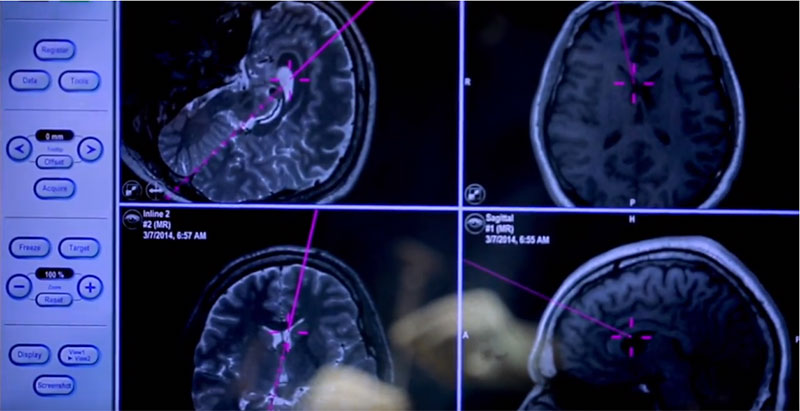
Frameless stereotaxy was used for all procedures for trajectory planning. Endoscopic cyst removal included a combination of aspiration, cyst wall dissection, bipolar coagulation, and, if necessary, a side-cutting edge device. At the end of the surgery, the procedures were identified as either complete or incomplete removal based on ventriculoscopic assessment by Dr. Souweidane. There was no difference in surgical resection technique in adults and children.
In total, 123 endoscopic resections were performed in 119 adult patients between the ages of 19 and 73 years old; nine endoscopic resections were performed in pediatric patients ranging in age from 9 to 18 years old. The results of their review included:
- Pediatric patients presented incidentally more frequently than adult patients (66.7 percent vs 37.4 percent).
- Of the adult patients with resections, 8 (6.5 percent) presented with acute deterioration.
- 67 percent of pediatric patients were asymptomatic at diagnosis.
- Frequency of hydrocephalus at presentation (11.1 percent vs 63.4 percent) was significantly lower in children than adults.
- Pediatric patients had a mean maximal cyst diameter of 8.7 mm compared to 11.8 mm in the adult group.
- Rate of complete cyst removal (88.9 percent vs 90.2 percent) was similar between adults and pediatric patients.
- Postoperative complications in adults included seizure, aseptic meningitis, ventriculitis, titanium burr hole cover dislodgement, and superficial wound infection.
- No recurrences or postoperative complications occurred in the pediatric group.
- Average length of stay was 2.9 days for adults and 1.6 days for pediatric patients.
The Weill Cornell Medicine researchers noted, “If pediatric patients tend to be less symptomatic than adults and their mean cyst size is smaller, the natural problem that physicians who manage these patients encounter is determining whether to treat. If treatment is indicated, questions arise regarding appropriate timing and optimal treatment modality.” They also point out that age must be considered in the decision to pursue prophylactic surgery due to the cumulative risk of tumor progression or acute deterioration.
Is There a Genetic Component?
Dr. Souweidane and his Weill Cornell Medicine neurosurgical colleagues regularly conduct research into colloid cysts and recently explored the possibility of an inherited predisposition to their development, the results of which were published in the April 2022 issue of the Journal of Neuro-Oncology.
Drawing on the Weill Cornell Medicine registry of patients with colloid cysts between 1996 and 2021, the researchers retrospectively collected data pertaining to a family history of colloid cyst. The rate of familial co-occurrence within that series was then compared to a systematic literature review and aggregation of familial case studies, as well as population-based prevalence rates of sporadic colloid cysts.
Thirteen cases with affected first-degree relatives were identified in the series. The majority of transmission patterns were between mother and child (9 out of 13). Compared with the estimated prevalence of colloid cysts, the familial colloid cyst rate of 13 cases in 383 (3.4 percent) estimates a greater-than-chance rate of co-occurrence.
The Weill Cornell Medicine researchers concluded that although this familial co-occurrence rate of 3.4 percent is likely an under-estimate of the prevalence of familial colloid cysts, this finding could provide a basis for establishing surveillance guidelines to encourage early recognition of this entity and possible treatment. Furthermore, identifying a transmission pattern may yield more insight into the molecular and genetic underpinnings of colloid cysts.