




When the Coarctation of the Aorta Stent Trial (COAST) was first introduced 15 years ago, its purpose was to determine whether stents were safe and effective in the treatment of native and recurrent aortic coarctation in selected children, adolescents, and adults. While surgery is the standard of care for coarctation of the aorta (CoA) in the neonatal period and in infancy, percutaneous treatment with balloon angioplasty and stent implantation are the methods of choice for growing children and into adulthood. But where do the analyses of long-term outcomes point? This is the question that COAST and COAST II have sought to answer.

Dr. Ralf Holzer
Ralf J. Holzer, MD, is the David Wallace-Starr Foundation Professor of Pediatric Cardiology at Weill Cornell Medicine, Chief of the Division of Pediatric Cardiology at NewYork-Presbyterian Komansky Children's Hospital, and Director of Pediatric Cardiac Catheterization at NewYork-Presbyterian/
The findings, published in the June 2021 issue of Circulation: Cardiovascular Interventions, demonstrated that coarctation stenting is generally effective at maintaining hemodynamic results over the 60-month follow-up period and decreasing the need for antihypertensive medication. However, the combined data from both COAST trials also indicated that risk for potential complications – stent fractures, aortic wall injuries, need for reintervention – persist and can develop many years later.
The combined data from both COAST trials also indicated that risk for potential complications – stent fractures, aortic wall injuries, need for reintervention – persist and can develop many years later.
While the there is a lack of prospective data comparing stent placement to alternative treatments such as balloon angioplasty or surgery, Dr. Holzer notes that there is some data that suggests that stenting has better results than the other treatment modalities. This is largely based on the findings of the prospective multi-institutional registry study by the Congenital Cardiovascular Interventional Study Consortium (CCISC), which compared stent implantation, balloon angioplasty, and surgery as treatment modalities for coarctation. That study, published in Catheterization and Cardiovascular Interventions in 2011, showed that stent implantation had shorter hospitalizations and fewer acute complications when compared to surgery; achieved lower upper to lower extremity blood pressure gradients; and was less likely to encounter aortic wall injury on follow-up when compared to balloon angioplasty.
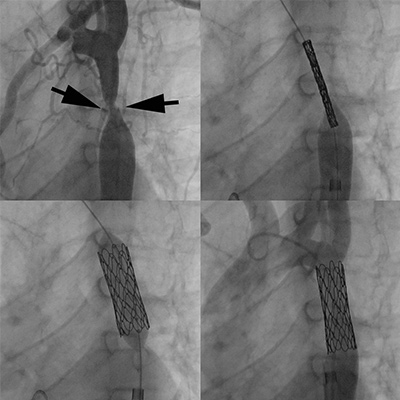
A 15-year old boy was born with a tight coarctation, which was relieved through implantation of a covered stent. (Top left image, in between arrows) documents the narrowing, with positioning of a covered CP stent (top right image). Stent expansion (bottom left) and final angiography documents complete relief of the narrowing with the vessel now wide open (bottom right).
“I believe some of the complications we continue to see from implanting stents in children are due to their ongoing growth and development,” continues Dr. Holzer. “In fact, some re-interventions are therefore not really complications of the procedure, but instead are anticipated elective treatments to expand stents to accommodate interval growth. Our current study is the largest prospective study to date with comprehensive follow-up data on outcomes up to 60 months and it did show that transcatheter treatment for the management of coarctation will likely have consequences down the line, most notably aortic wall injury.”
Specifically, the 2021 study combining data from COAST, COAST II, and their Continued Access extensions, showed for late follow up (48-60 months):
- Incidence of stent fractures – 24.4 percent
- Need for reinterventions – 21.3 percent
- Incidence of aortic wall injury – 6.3 percent
“While this four- to five-year data is important, longer-term data is really crucial,” notes Dr. Holzer. “What I want to know is when you put these stents in patients early in life, what happens once they're fully grown. Does the incidence of aortic wall injury continue to rise or is it expected to plateau? Will the need for re-intervention decrease? These patients should have a CT angiography of the aorta to look for the possibility of an aneurysm, which won’t necessarily show up on an echo or MRI exam. Stress testing is important to evaluate blood pressure response to exercise, as hypertensive exercise responses may not be evident on standard blood pressure readings taken in the clinic. The current data tells us the jury is still out on how these patients with stents will do in the long term.”
“While the four- to five-year data is important, longer-term data is really crucial. What I want to know is when you put these stents in patients early in life, what happens once they're fully grown.” — Dr. Ralf Holzer
With this in mind, Dr. Holzer has proposed a longer-term outcome study of the Coarctation of the Aorta Stent Trials with similar objectives: to identify outcomes – aortic wall injury, reinterventions, hypertension incidence and management – at least 10 years following stent implantation, to compare the results to earlier follow-up data, and to identify possible predictors of late-term outcome post-stent implantation.
“From a clinician standpoint, it would be of great benefit to know if fractures, need for reintervention, and aortic wall injury would eventually plateau and stenting delivers a more sustainable long-term outcome by 10 years,” says Dr. Holzer. “If we learn that adverse outcomes do not escalate and the number of patients we see with aneurysms or requiring reinterventions declines, this would not only make a more persuasive case for using stents over surgery, but also having outcomes data on complications over the long term lets us know how frequently we need to follow patients to keep an eye out for potential problems that may develop. It also enables us to set realistic expectations when talking to patients and parents before any intervention.”