


NYC-SIGHT: Facilitating Eye Health Screenings and Follow-up Eye Care in Vulnerable Populations
NewYork-Presbyterian/Columbia is one of three institutions leading community-based efforts to address glaucoma and other eye issues. In 2019, the Vision Health Initiative of the Centers for Disease Control and Prevention funded three five-year research grants to develop innovative vision screening strategies for high-risk populations. Funding supported Screening and Intervention for Glaucoma and eye Health through Telemedicine (SIGHT) studies, which are taking place in New York City, Alabama, and Michigan.
Lisa A. Hark, PhD, MBA, Professor of Ophthalmic Sciences at Columbia and Director of the Ophthalmology Clinical Trials Unit at NewYork-Presbyterian/Columbia, was named the principal investigator of NYC-SIGHT and the coordinating center for the three sites. “The Alabama site conducted screenings in primary care settings in a rural environment,” says Dr. Hark. “The Michigan site focused on federally qualified health centers. And here in New York, we were going directly into the communities where people live.”

Dr. Lisa Hark
“One of the major issues is follow-up by participants following an eye health screening,” says Dr. Hark. “You can identify individuals who have a vision problem that needs care, but many people just fall through the cracks. They don’t follow up with an ophthalmologist or optometrist. They don’t make an appointment, or they don’t have an eye doctor to even call if they have blurry vision or worry about their eyes.”
According to the National Institute of Minority Health and Health Disparities and studies published in JAMA Ophthalmology and the American Journal of Ophthalmology, minority, socioeconomically disadvantaged, and underserved urban and rural populations are disproportionately affected by eye disease. Diabetic retinopathy, glaucoma, and vision impairment appear more frequently in communities with a large number of residents living in poverty, older adults, and those who are Black or Hispanic.

Dr. Jason Horowitz
“Most people know that it is important to have eye care to prevent permanent damage that can’t be fixed down the road, but they have trouble navigating the healthcare system even under the best of intentions and circumstances,” says Jason D. Horowitz, MD, Associate Professor of Ophthalmology at Columbia and Medical Director of the Ambulatory Care Network Eye Clinic at NewYork-Presbyterian/Columbia. “This is true for people in all walks of life.”
With funding from the Vision Health Initiative, Dr. Hark and her colleagues developed – in collaboration with the New York City Housing Authority (NYCHA) and the NYC Department for the Aging (DFTA) – the Manhattan Vision Screening and Follow-up Study (NYC-SIGHT).
“Our premise was that taking the eye health screening program into the Washington Heights and Harlem communities would not only facilitate access to eye care, but also enable us to improve adherence with follow-up eye care,” says Dr. Hark. “The neighborhoods within the NewYork-Presbyterian/Columbia catchment area include large public affordable housing developments with senior centers, community centers, and gymnasiums, for example, where large eye health screenings could be held. Our goal was to determine what is the range of pathology of eye disease in this community and how can we get individuals into eye care to prevent blindness.”
The Manhattan Vision Screening and Follow-up study is the first community-based study in New York City targeting residents living in affordable housing to detect glaucoma and other eye diseases in a predominately older, African American, and Hispanic population.
NewYork-Presbyterian/Columbia is located in the Washington Heights/Inwood section of Upper Manhattan– an area with more than 200,000 residents with a racial/ethnic composition comprised of 2.5 percent Asian, 7.9 percent Black, 67.9 percent Hispanic, and 19.2 percent white, and a poverty rate of about 15.5 percent. “At least 70 percent did not have access to an eye doctor, 50 percent had not had an eye exam in the past two years, and too many never had an eye exam,” Dr. Hark stated.
The researchers recruited individuals at-risk for eye disease who were living at or below the New York City poverty measure in Washington Heights and adjacent neighborhoods in Harlem. The study involved 10 affordable housing developments, with a potential target group of 6,000 NYCHA residents over the age of 40. The goal of the NewYork-Presbyterian/Columbia research team was to determine if community-based eye health screenings in adults and seniors can improve early detection and management of glaucoma, vision impairment, cataracts, and other eye diseases, and whether patient navigators can improve access to ophthalmologic care in these high-risk populations.
Columbia’s eye health screening included:
- Visual acuity with correction
- Intraocular pressure (IOP) measurements
- Fundus photography
“We provided more than a vision screening,” says Dr. Hark. “Normally a screening involves visual acuity check using the Snellen eye chart and IOP testing, and if high, indicates a risk to check for glaucoma risk. Our process also included fundus photography using a hand-held camera to examine the retina (without dilation) to determine the presence of ocular diseases. This is a unique aspect of our program and did not require dilation.”
Dr. Horowitz, who oversees the retinal imaging component of the study, concurs. “One of the exceptional components of our screening was conducting fundus examinations with a portable camera that enabled us to do a deeper dive into diagnosing eye disease. We took six images per person – three images of the right eye and three images of the left eye. Over 4,000 images were sent to Columbia and loaded into the image reading software, enabling the eye doctors to read those images remotely. We found 26 percent of 700-plus people in the study had glaucoma or clinical features suggesting glaucoma – which is enormous – and needed to get into eye care.”
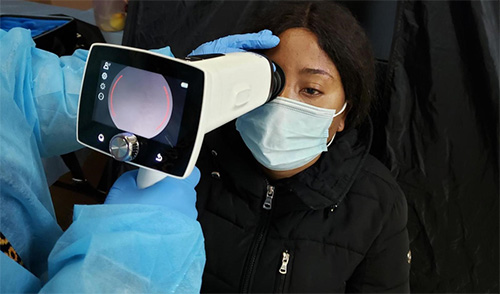
A screener uses a portable camera to view the interior surface of the eyes of a study participant. Photo courtesy of Lisa Hark.
An Innovative Strategy for Eye Health Screening
A total of 708 participants 40 years and older completed the eye health screening in various NYCHA community settings and senior centers between March 1, 2021 to May 31, 2022. Participants were randomized to an Intervention Group (454 participants) or a Usual Care Group (254 participants). Those in the Intervention Group received free eyeglasses and, if they were referred to ophthalmology for follow-up care, they were assisted by patient navigators for one year. The individuals in the Usual Care Group were given a prescription for eye glasses and names of local optical shops, but if they were referred to ophthalmology, only the initial eye exam appointment was made for them and no assistance was provided by patient navigators.
“We reduced a lot of the barriers to screening for participants,” notes Dr. Hark. “We conducted the screening in their local community, which was extraordinarily convenient. We helped them make an appointment, and if they didn't show up, we helped them to reschedule. We didn't ask them for their insurance. The screenings were free. We also scheduled follow-up appointments for those referred to ophthalmology.
Baseline results, published in the January 23, 2023, online issue of the American Journal of Ophthalmology, included:
- Study participants were 51.8 percent African American and 42 percent Hispanic.
- A total of 555 participants (78.4 percent) failed the eye health screening.
- 497 had visual acuity (VA) of 20/40 or worse; 49 had intraocular pressure (IOP) >23 mmHg.
- Within three weeks of the eye health screening, 365 participants were scheduled to see the on-site optometrist due to VA 20/40 or worse, IOP 23-29 mmHg, or an unreadable image, and 83% attended this eye exam in the same location.
- Overall, 468 of the 708 screened participants (66.1 percent) were referred to ophthalmology for follow-up.
- Study ophthalmologists’ telemedicine image reading based on the worse eye showed 281 participants (39.7 percent) were normal or abnormal with no significant findings; 175 (25 percent) were unreadable and referred to the optometrist; and 250 (35 percent) had an abnormal image and were referred for further ophthalmological evaluation.
- Participants identified with glaucoma or glaucoma suspect (n = 138) and retina abnormalities (n = 157) seen on fundus images were referred to ophthalmology; 7 subjects had an IOP >30 mmHg and were fast-tracked; 5 of the fast-tracked participants also had an abnormal image.
- Of those participants with an abnormal fundus image, 62 passed the routine screening and would have been missed without this imaging.
- Both the Intervention Group (free eyeglasses) and Usual Care Group (eyeglass prescription only) had a high show rate for on-site optometric exam appointments (86 percent and 80 percent, respectively), suggesting that this on-site eye exam was an important service.
- 103 participants were referred by the optometrist for an annual dilated eye exam because they never had an eye exam or had not seen an eye doctor within the past two years.
- 95.3 percent of participants had health insurance: 57.2 percent Medicare, 54.9 percent Medicaid.
- The cost per participant to deliver the eye health screening and optometric exam was $180.88; the cost per case of eye disease detected was $273.64, primarily related to staff expenditures.
“As a result of Dr. Hark and her team’s efforts, a considerable number of individuals have been screened with many found to have significant eye problems warranting a referral to physician care,” says Dr. Horowitz. “At the heart of this research is deciding how much to help people obtain access to eye care and how should resources be invested to achieve the best possible outcome. There are various degrees of facilitation. For example, you can tell a patient they have a bit of high pressure and should make an appointment to see a particular ophthalmologist, which is valuable information. Or you can provide more extensive support, such as making the appointment for them and ensuring they get to the appointment. That’s a higher level of facilitation. And while we think that approach is better, we also recognize that it requires a significant additional commitment of resources.
“This scientific study is important to demonstrate how much visual difference is there for this incremental and active facilitation of resources,” continues Dr. Horowitz. “Our research is providing important evidence to help answer these questions. Along the way, we have screened many patients and helped a lot of patients get access to needed eye care. That’s a great positive. But the bigger picture is that when the final results are analyzed, we are going to see how much those extra resources contribute to a superior visual outcome compared to conventional screening approaches.”
Vision for the Future
The Manhattan Vision Screening and Follow-up Study is now in its fourth year. Based on the preliminary results from this study, Dr. Hark will be seeking additional funding from the National Eye Institute and CDC to pursue a second phase of the study beginning in 2024 for a period of five years. The new study would focus on younger people, ages 18+, and extend the geographic area covered, thereby increasing the potential pool of participants from 6,000 to 30,000. “We want to scale the program to the larger NYCHA developments in upper Manhattan and make it more available to individuals who are working by offering the eye health screenings on Fridays and Saturdays,” notes Dr. Hark.
Read More
Manhattan Vision Screening and Follow-up Study (NYC-SIGHT): Baseline Results and Costs of a Cluster-Randomized Trial. Hark LA, Horowitz JD, Gorroochurn P, Park L, Wang Q, Diamond DF, Harizman N, Auran JD, Maruri SC, Henriquez DR, Carrion J, Muhire RSM, Kresch YS, Pizzi LT, Jutkowitz E, Sapru S, Sharma T, De Moraes CG, Friedman DS, Liebmann JM, Cioffi GA. American Journal of Ophthalmology. 2023 Jan 20:S0002-9394(23)00028-4. [Online ahead of print]
SIGHT | Screening and Intervention for Glaucoma and eye Health through Telemedicine
For More Information
Dr. Lisa Hark
Dr. Jason Horowitz
NewYork-Presbyterian
Advances in Ophthalmology
Read more about our latest clinical advances.