




Despite coronary artery disease being highly prevalent among women, in research of the disease, females are often under investigated, under treated, and have less favorable outcomes. “Previous reports with atherectomy have shown that females with calcified coronary artery disease are more susceptible to adverse procedural outcomes compared to males,” says Margaret McEntegart, MD, PhD, Director of the Complex Percutaneous Coronary Intervention Program at NewYork-Presbyterian/

Dr. Margaret McEntegart
Recent studies suggest that intravascular lithotripsy (IVL) for coronary artery calcification using the Shockwave C2 coronary IVL catheter device produces similar safety outcomes for men and women. However, the existing research fails to adequately represent the female patient population with this condition. “Women tend to present with atypical symptoms or less classical symptoms of ischemia,” notes Dr. McEntegart. “In addition, we know that women have smaller or more tortuous vessels. When we look at the published studies, there is a lower use of intravascular imaging. All of these factors taken together result in a higher complication rate during the procedures, particularly complications such as perforations and extensive dissection.”
To address these discrepancies, Dr. McEntegart, an interventional cardiologist, and Alexandra Lansky, MD, Director of the Heart and Vascular Clinical Research Program at Yale University School of Medicine, are serving as co-principal investigators for the EMPOWER CAD study. EMPOWER CAD is a prospective, multicenter registry that seeks to enroll up to 400 female patients with symptomatic ischemic heart disease across some 50 investigational centers in the United States and Europe with at least a three-year follow-up of patients. Through this study, Dr. McEntegart and the research team seek to determine if the safety results from the earlier IVL studies representing men and women could be replicated in an all-female population.
“EMPOWER CAD will be different from other studies because it will be an all-female patient study conducted by two female PIs,” says Dr. McEntegart. “We’re also going to have a high prevalence of female site investigators. In doing so, we are hoping to provide experience for female interventional cardiologists who wish to develop their skills and experience in clinical trials and who as yet have not had the opportunity to do so.”
IVL was established on the principles of kidney stone treatment and adapted for calcium in the cardiovascular system. A series of miniaturized lithotripsy emitters are arrayed within a balloon angioplasty catheter to create a localized field effect at the site of the calcium. These emitters deliver controlled pulsatile waves to break up the calcium deposits into smaller pieces that can be more easily displaced to facilitate stent implantation.
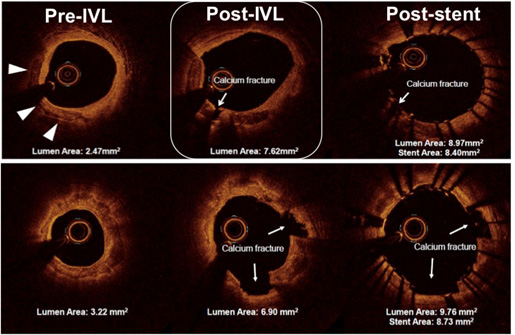
Optical Coherence Tomography showing calcium inside a coronary artery, the fractures created by lithotripsy, and stent expansion after lithotripsy treatment.
(Courtesy of Dr. Margaret McEntegart)
Dr. McEntegart notes the study is an important opportunity to improve care for females with coronary artery calcification. “We know that when women have calcium in their arteries, it is an independent predictor of poor outcomes,” she says. “And we know when we try to treat the calcium, these patients are exposed to higher risk from the treatment. There is an immediate and unmet clinical need for determining the safest treatment strategy for women with severely calcified coronary lesions. The idea that a device could provide effective treatment without exposing these female patients to excessive risk is quite an exciting prospect.”
Despite often being more challenging to treat, female patients are under represented in published data, and there have been no dedicated prospective studies performed on this population. This is the first-ever prospective coronary revascularization study consisting of all female patients.
— Dr. Margaret McEntegart
Addressing Gender Disparity in Cardiovascular Research
EMPOWER CAD also serves to improve research representation of women in patient populations for cardiovascular disease. Most cardiovascular research has focused on men despite women representing roughly half the general population and despite heart disease being the number one cause of death in women. “There’s a real shortage of data about how to manage female patients,” notes Dr. McEntegart. “So far, we’ve relied on extrapolated data from the male population and assumed that the way we’ve treated coronary disease in men will have the same outcomes in women. We’re only recently becoming very aware of the fact that when you look into most of the trials, the inclusion populations are only about 10 to 20 percent females, even in contemporary studies. So, we’re still not including women in a lot of these big cardiovascular trials.”
Cardiologists are only just coming to terms with this disparity and its fundamental effect on how they diagnose and treat their patients. “It’s interesting that as a female physician, at some point you realize that you’re also biased because you’ve been trained on data based on men,” says Dr. McEntegart. “For instance, in medical school we were taught the classic symptoms for a heart attack: pain or pressure across the chest, around the back, down the left arm, and up into the jaw. But we now understand that women don’t always present with these symptoms. They often present with more subtle signs such as breathlessness or fatigue.”
Dr. McEntegart feels strongly that addressing this research gap will benefit patients and providers alike. She hopes the EMPOWER CAD study is an indicator of research to come. “The fact that this is a female-only trial is quite a signal of intent,” she says. “Going forward, we need to drive appropriate levels of recruitment in larger trials and conduct additional female-specific trials where there is a difference in therapeutic safety or effectiveness between men and women. This trial is a fantastic start.”
